
Wow, this is an embarrassing article to …
write. Oh, I don’t mean that writing an article on the human vagina is embarrassing. After all, as a physician, I deal with this organ and its associated diseases on a regular basis. No, the article is embarrassing to write because it is about a complex problem occurring in the vagina that is commonly misdiagnosed and improperly treated by clinicians, including internists, family physicians, and OB/GYNs, all who should have a high level of expertise in this area. It’s embarrassing because when I see patients with this issue (and sometimes other complex vaginal disorders), the problem has often gone on for years and multiple clinicians have missed it. There have been repeated, rushed office visits, the usual clinical bravado that doctors and mid-level providers use on patients to hide their discomfort over a bewildering condition, and incorrect treatment. I consider every diagnosis that I miss to be an important, painful, and significant learning opportunity. So, too, are diagnoses that others have missed. My objective here is to educate interested patients directly.
The 70s rock band Nazareth might have sang, “Love Hurts,” but sexual intercourse should not hurt. If you are a woman and sex is painful, you have a medical problem that most likely can be fixed. This may seem pretty basic, but I can’t emphasize it enough. Sex should not be painful. Many conditions can cause painful sex. Some are more challenging than others.
The painful sexual disorder I’d like to address this time is called vaginismus (Vag-IN-iss-muss). Vaginismus is a disorder where the muscles around the vagina fail to relax during intercourse. The medical literature often wrongly describes this failure to relax as a “spasm,” but that is not the case. The human vagina constantly maintains a modest amount of muscular tone in the non-sexually aroused state. Normally, when a friendly penis approaches the vagina, the vaginal muscles relax. If they don’t relax, then sex is painful. Think about your anus, as many of us do from time to time. It constantly keeps a bit of muscular tension but relaxes when it needs to. It is a similar phenomenon. But here is one important difference. Whereas the muscles around the anus encircle it entirely, the muscles which fail to relax near the vagina occur only in the lower part, and by “lower” I mean only that part of the vaginal opening which is closest to the anal opening. If you are looking at the vagina as if it were a clock, the area of concern is in the 5:00 to 7:00 position. Consult the diagram to see where muscles need to relax to permit intercourse comfortably. In vaginismus, the vagina does not shut down completely, as you would if you were squeezing closed your anus. Instead, it is just the lower portion that fails to relax. Try this exercise to simulate the condition. Make your mouth like a relaxed, medium-sized “O.” Now, tense up only your lower lip. That is vaginismus.
When a clinician is doing a pelvic exam, it is possible to diagnose this condition. As part of inserting the speculum into the vagina, the clinician should put a finger slightly into the vagina and press downward toward the floor. In a normally functioning vagina, this downward pressure will cause the vaginal muscles to relax and make insertion of the speculum easier. If those muscles on the lower end of the vagina (again, closet to the anal opening, and furthest from the clitoris) fail to relax, there are three possibilities. The first is that this woman really, really hates having a pelvic exam. If she enjoys intercourse and does not find it at all painful to have a penis in there during sex, then this is just a response to the setting of the pelvic exam. The second is that she is a virgin. In virgins, those vaginal muscles will not relax until she’s had sex and her vagina figures out that sex feels good and muscles should be relaxed during intercourse. Virgins should almost never need a pelvic exam anyway. A third possibility is vaginismus. If she cannot sit still on the exam table, raises her buttocks, pulls in her knees, or otherwise cannot cooperate with the exam and she is a non-virginal female, then this may represent vaginismus.
 Medical textbooks often portray this condition inaccurately. Phrases such as “involuntary muscle spasm” are very misleading. If I have an “involuntary muscle spasm” in my back I am probably rolling on the floor in agony. “Contraction of the vagina” makes people wrongly think that the vagina is shut totally closed like the anus. Both of these characterizations are wrong. It is the failure of the vagina to give up its normal, constant mild muscle contraction in its lower, or 5:00 to 7:00 position, which is the hallmark of this disorder. Now, certainly if you try to insert something into the vagina of a vaginismus patient, it may contract a bit more strongly. Try this: feel your biceps muscle in the totally relaxed state. Now contract it mildly. This is the normal muscle down in the lower part of the vagina. Now contract it harder. This is the response of the muscles of a vaginismus patient at the lower vagina to an attempt to insert a penis. The muscle contraction itself is not painful at all. It is when a penis pushes on this contracted vaginal muscles that pain ensues.
Medical textbooks often portray this condition inaccurately. Phrases such as “involuntary muscle spasm” are very misleading. If I have an “involuntary muscle spasm” in my back I am probably rolling on the floor in agony. “Contraction of the vagina” makes people wrongly think that the vagina is shut totally closed like the anus. Both of these characterizations are wrong. It is the failure of the vagina to give up its normal, constant mild muscle contraction in its lower, or 5:00 to 7:00 position, which is the hallmark of this disorder. Now, certainly if you try to insert something into the vagina of a vaginismus patient, it may contract a bit more strongly. Try this: feel your biceps muscle in the totally relaxed state. Now contract it mildly. This is the normal muscle down in the lower part of the vagina. Now contract it harder. This is the response of the muscles of a vaginismus patient at the lower vagina to an attempt to insert a penis. The muscle contraction itself is not painful at all. It is when a penis pushes on this contracted vaginal muscles that pain ensues.
A woman with vaginismus can have sexual intercourse. She will get aroused if she is dating George Clooney or Leonardo DiCaprio, and her vagina will lubricate normally. The patient wants to have sex, but when a penis touches the outer portion of her vagina, those lower muscles fail to relax and may contract a bit more strongly. In some women, the vaginismus is so strong that no penis can enter. In many cases, however, a penis will be able to enter, but the experience is uncomfortable, described as burning, sore, or otherwise painful.
Woody Allen once joked that he was one of the few males to suffer from penis envy. Although, I don’t have a vagina, I do hate going to the eye doctor. I’m often amazed at how some patients can cooperate with an eye exam. When I am the patient and that brutish ophthalmologist comes at me with the gizmo to check my intraocular pressure (known as a Schiotz Applanation Tonometer), my eyelid goes into spasm and I can’t sit still in the chair. It is nearly impossible to get a good reading on me. Even those air puff devices are a challenge because I am so worked up over the idea of a puff of air on my eyeball. You might say I have vaginismus of the eye.
When a female patient is undergoing a pelvic exam and she is unable to relax her vagina, the exam is more uncomfortable than it might be. She may be quite restless on the exam table, unable to sit still, or push her pelvis away. A common error from clinicians is to tell her to relax or admonish her for not putting up with the exam. It is almost “Saturday Night Live” worthy to imagine a physician and a nurse shouting at a patient to relax in this setting, but I’m sure it happens in real life. The correct action is to immediately inquire if intercourse is painful. If her difficulties are truly limited to a pelvic exam, then perhaps no real disorder is present, but if intercourse is also painful, then vaginismus is a potential diagnosis. Clinicians (and patients) need to not be afraid of the contraction of that vaginal muscle, which we call the pubococcygeus muscle. Get a finger on it. Use your thumb on the outside as well. Doctors and patients should not make the error of thinking the vaginal opening is too small for intercourse. That tensed pubococcygeus muscle might feel like a firm lump of muscle tissue, but it is not truly a lump. It will disappear with relaxation of the relevant muscles.
If the most common error is missing vaginismus entirely, the next error is to assume that this disorder has some sort of deep seated psychological roots. In most cases, it is simply a normal neuromuscular reflex present in virgins which has not extinguished itself as it should in a sexually active woman, or it has re-developed owing to some other painful vaginal problem.
Primary vaginismus is when the vagina never made the transition from a virginal vagina to a sexually active vagina. Secondary vaginismus is when the vagina used to relax normally but now no longer does. Sometimes this is a result of some other condition which causes pain with intercourse, so now there are two reasons for sex to hurt. A woman is not to blame for having vaginismus. She has no more voluntary control over this reflex than I do over keeping my eye open at the eye doctor.
The best way to treat
vaginismus is with
a series of vaginal dilators.
The best way to treat vaginismus is with a series of vaginal dilators. These look like a robot penis, shaped roughly like a penis, but without any of the personality (see picture). Depending on the severity of the condition, a woman starts with a small dilator or even a Q-tip. Some women are so sensitive that a bit of numbing jelly is needed, but others don’t need that. The small dilator is put into the vagina and left there. If it hurts, you need a smaller dilator. The goal is to teach the vagina that it is not painful to have an object inside. When the dilator is inside and not painful, it is time to occupy yourself by just lying there, reading War and Peace, watching TV, or falling asleep. If you have a partner, this is a great time to make out, but obviously, there should be zero attempts at intercourse until the patient has slowly worked up to the largest, Mr. T sized dilator and can insert it and leave it there without any discomfort. Patients can masturbate with the dilator in place as another mechanism to train the vagina that it is okay to have an object in there during sexual arousal.
A set of dilators and a great instructional DVD is available from www.vaginismus.com. I recommend the full $99 package which has the dilators, video, and the instruction book. The video was shot in the 1970s and it is both very instructive and also hilariously campy. Two thumbs up.
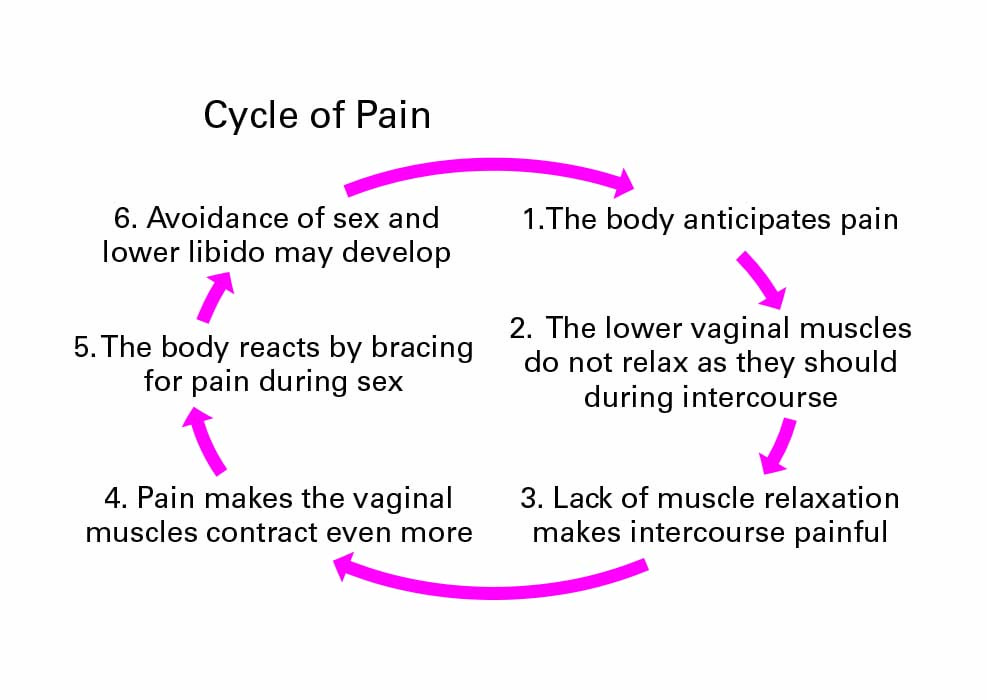
A second problem that can occur with vaginismus is that the long term association with painful intercourse will sometimes, but not always, lower a woman’s sex drive considerably. The lowered libido in this setting is addressed with other techniques, most commonly sensate focus exercises which were the topic of a prior article. A slightly modified approach is needed in the setting of vaginismus.
If you have pain with sex, you should come see me, or of course you are welcome to go and see your OB/GYN if you prefer and if that person can’t fix your problem, then come see me. Although vaginismus is only one of the many causes of painful intercourse, it is often missed but almost always treatable when we make the right diagnosis.